
RESOURCES
The Library
Since 1992, PMRG has helped and guided ophthalmologists to navigate the sometimes difficult waters of running a physician owned medical practice. Over those years, we have written and published many articles in support of that work. This library of offerings is updated and added to regularly and is here as a resource to assist you in the operations and management of your practice.
Please come back often and don’t hesitate to let us know if there is something you would like us to write on that is not listed here!
To contact us to find out more or to suggest a topic, please click here.
In today’s competitive healthcare environment, patient experience is a major differentiator. From routine exams to complex surgical care, patients expect convenience, efficiency, and clear communication at every stage. Practices that prioritize access and experience improve satisfaction, retention, referrals, and overall growth.
In today’s evolving healthcare environment, ophthalmology practices must balance exceptional clinical care with strong financial performance. As reimbursement models grow more complex and patient responsibility continues to rise, optimizing Revenue Cycle Management (RCM) is essential to maintaining profitability, compliance, and long-term sustainability.
The healthcare landscape is evolving faster than ever. For those of us running busy practices, simply maintaining the status quo is no longer a viable strategy. As we turn our attention to 2026, setting clear, impactful strategic goals is paramount to ensuring financial health, operational efficiency, and superior patient care. A well-rounded strategic plan shouldn't just focus on revenue; it must address the patient experience, staff development, and technological adoption.
Click to see a framework to kickstart your own 2026 Strategic Goal planning session!
All-Payer Claims Databases (APCDs) are large state-managed databases that collect healthcare claims data from both public and private insurers. These databases include medical, pharmacy, and dental claims, as well as eligibility and provider files.
The landscape of healthcare is in constant motion, and managing an ophthalmology practice today presents a unique set of complexities. In this dynamic environment, PMRG is your partner, offering expert consulting services.
Emergency Action Plans (EAPs), while sometimes voluntary and sometimes required for medical practices, are a crucial step in ensuring the safety and well-being of both employees and patients.

The Stone Oak Ophthalmology Center, a three-provider practice based in San Antonio, Texas, came on board with PMRG as their billing service provider in 2019.
After 3 years of solid work and a strong partnership with PMRG, Dr. Allison Young, the practice founder, was drawn away by the promise of having their EPM, EHR, and billing service all under one company.
It didn’t take Dr. Young long to realize that she had made a mistake.

This article explains when to use VSP as a secondary or tertiary insurance; how to bill it; and how to communicate this benefit effectively to patients.
Are you thinking about switching things up and changing your practice management (PM) system, your EMR or both? If you are, you’re not alone! It is important to understand the ramifications of doing so before you get started.
Understanding your payer contracts can affect denial of payment as well as the amount and timeliness of reimbursement. Learn more about the provisions you should consider when reviewing potential new or existing payer contracts.
Many of you may be aware of the CMS evaluation and management add-on code that was introduced in January of this year. According to CMS, “G2211 captures the inherent complexity of the visit that’s derived from the longitudinal nature of the practitioner and patient relationship”.

Social Determinants of Health (SDoH) are economic or social conditions in the environment that can affect individuals’ health and quality-of-life outcomes.
Consolidated billing was established by the Centers for Medicare & Medicare Services (CMS) in 1998 to help eliminate duplicate billings for services rendered to SNF residents by multiple providers. With consolidated billing, an SNF receives a basic per diem rate per level of care for each resident.
There are times when care is not covered by Medicare because they deem the service not medically necessary. In these circumstances, it is vital to make sure that you communicate the likelihood that the service will not be paid for by Medicare and give your patient the option to receive these services but pay for them out-of-pocket.
This communication is called an Advanced Beneficiary Notice of Non-Coverage, or ABN.
National Coverage Determinations (NCDs) and Local Coverage Determinations (LCDs) are created by the Centers for Medicare & Medicaid Services (CMS.) They apply to all Medicare providers to establish how a service will be covered; what criteria is required to establish medical necessity; and what documentation requirements there are for the service.
Time management is the organization of one’s time and activities. Time-management skills are important for health care professionals who must perform a multitude of different tasks throughout the day.
Collecting patient balances at the time of service is a key step in your revenue cycle. If your office does not currently have policies and procedures in place for collecting from your patient at the time of the visit, it can be a challenge to implement.
Although it may seem the easiest way to be “compliant, if your compliance plan is not personalized for your practice, you could face scrutiny from the OIG.
Patients with vision plans will sign a form at the time of service that explains that medical insurance may also be billed when necessary (Regarding Vision & Medical Insurance.)
Building, updating, and maintaining your contracted allowables for the major insurance carriers you are contracted with is a crucial aspect of managing a well-run practice.
It can be difficult to know what data your practice should be tracking. Most current practice management systems have such in depth reporting capabilities, it can be challenging to find a report or reports to quickly summarize your practice’s data to analyze your metrics and ensure business goals are being met.

Patients with vision plans will sign a form at the time of service that explains that medical insurance may also be billed when necessary (Regarding Vision & Medical Insurance.)
Comparative Billing Reports (CBRs) summarize Medicare claims data and distribute it to providers to provide insight into billing trends. Each CBR is unique to a single provider and is only available to that individual provider. CBRs are not punitive and will not be publicly available.
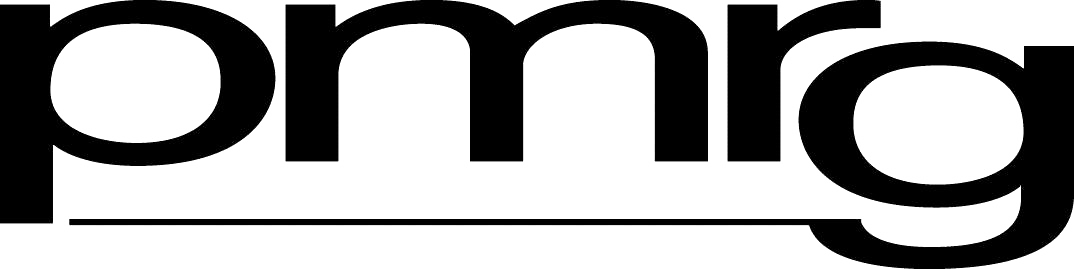
The August/September 1999 issue of Watching Your Bottom Line discussed evaluation of your practice’s fee schedule based on the use of the Resource-Based Relative Value Scale (RBRVS).
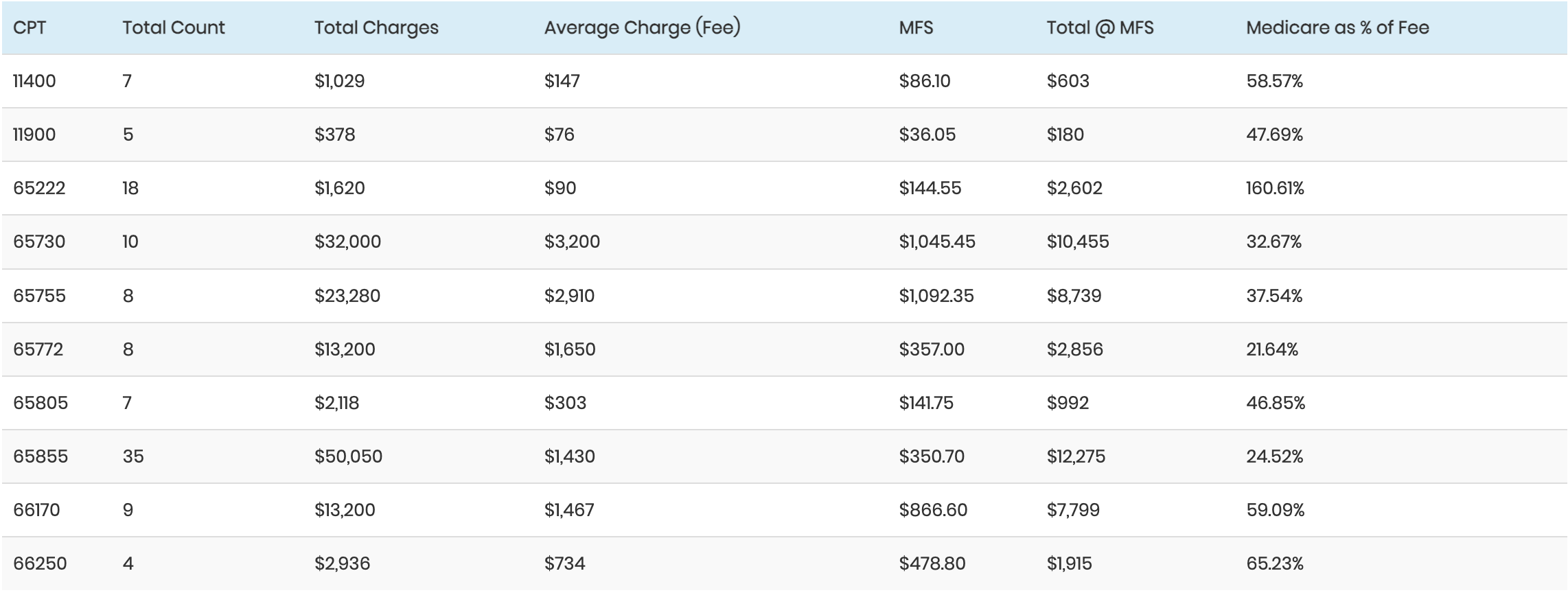
We’ve looked at charge capture, at productivity and product-line analyses, and at payor mix. We’ve also looked at how our computer systems handle and report data to ensure that we’re getting an accurate picture of our clinical activity translated into financial information. In this issue of the newsletter, we’ll put all of the income data together to calculate a collection target.

Usually a computerized billing system captures and reports information differently from the way you manage your practice’s business. Unless you build a customized program, you will have to understand your computer’s thinking in order to maximize its use as a management tool for your business.
Transforming a clinical service into income requires managing tens of thousands of transactions with hundreds of thousands of data elements. In order to make the difference between mediocre and outstanding collection performance, an effective and efficient billing process is required.
As the practice owner (or manager), one of the most powerful points of leverage you have for having your practice be effective and successful is your staff.
Implement systems to assure that an appropriate charge is entered for each clinical service. Use your computer system’s appointment scheduling to compare appointments with charge tickets, identifying missing tickets.

In the last issue we laid the groundwork for a monthly reporting package. We showed how to prepare reports of clinical activity and patient type. In this issue we’ll use the data from those reports in describing the reporting of collection performance, accounts receivable (AR), and practice expense.